Super Curcumin C3 Complex Wins Whole Foods Magazine Award!
Recently AFI’s Super Curcumin C3 Complex has won an award given out by Whole Food’s Magazine. The award was for the best immune health supplement.

Recently AFI’s Super Curcumin C3 Complex has won an award given out by Whole Food’s Magazine. The award was for the best immune health supplement.

Sports nutrition is a constantly evolving field – we understand it better because of the outpouring of results from thousands of research studies that are conducted annually. Finding sports nutrition products and ingredients that have proven studies to support claims of performance enhancement and energy in this field can be challenging, as unsubstantiated claims typically cloud the marketplace. We will list and discuss products in this review that have human clinical trial data at improving energy, endurance and other sports nutrition goals.
Sports nutrition supplements typically contain carbohydrates, fats, proteins, vitamins, minerals, herbs, and sometimes plant extracts. Supplements can generally be classified as convenience supplements such as ready to drink supplements, energy bars and meal replacement powders. They provide a convenient means of meeting caloric needs, while also delivering performance enhancement supplements.
Performance enhancement supplements that have science behind them include ergogenic agents such as caffeine, guarana, creatine, green tea extracts, willow bark, Kola nut, Sida cordifolia, Citrus aurantium (bitter orange), calcium and sodium phosphate, thyroid stimulators, including guggulsterones, black pepper extracts, and ginger root.
Plant-based supplements that are used in formulations include Tribulus terrestris (puncture weed or caltrops) and Fenugreek seed extract (Trigonella foenum-graecum), extracts that stimulate the natural production or release of bound testosterone to free testosterone. Free testosterone is the only metabolically active form of testosterone.
Both Tribulus and Fenugreek seed extracts have been marketed to promote greater gains in strength and muscle mass during weight training with sufficient clinical trial data to prove their efficacy.
Dietary calcium has been shown to suppress fat metabolism and weight gain during periods of high caloric intake. Further, increasing calcium intake has been shown to increase fat metabolism and preserve thermogenesis during caloric restriction.
The role of sodium and calcium phosphate on energy metabolism and exercise performance has been studied over several decades of research. Phosphate supplementation may influence metabolic rate possibly by affecting thyroid hormone levels. Phosphates could serve as potential thermogenic nutrients in supplement formulations.
Phosphates are formed during the Krebs cycle for energy production. Each turn of the Krebs or Citric acid cycle generates one guanosine triphosphate molecule which has a high-energy phosphate bond, stored energy that can then be broken to release energy for the cell.
Other Krebs cycle intermediates that have been used in sports nutrition include creatine phosphate, alpha-keto glutarate (AKG), sodium pyruvate and ethyl pyruvate. Creatine supplementation has, by far, the largest clinical trial documentation at increasing energy and enhancing athletic performance, although there is evidence that it loses its efficacy after long term use.
Green tea is believed to increase energy expenditure by stimulating brown fat (adipose) tissue thermogenesis. Green tea supplementation in combination with caffeine increased 24-hour energy expenditure and fat utilization in humans. The thermogenic effects of green tea supplementation depend on the synergistic effects of the caffeine and EGCG (epigallocatechin gallate) contents.
Other reported sports nutrition extracts include Rhodiola rosea, Eleutherococcus senticosus (formerly called Siberian ginseng) and Schizandra chinensis (Schizandra dried berries or extracts). These are all classified as adaptogens, since they allow the plants that produce them to survive in the Siberian tundra, where freezing and drought conditions occur on a regular basis.
These extracts are also called Russian adaptogens. The clinical trial data was compiled by Russian scientists beginning in 1947 through the 1970’s, but Western clinical double-blind or placebo-controlled standards were not used, which makes the data obtained from the studies of questionable value.
Schizandra chinensis does have the most compelling clinical data – it acts as a central nervous system stimulant or ergogenic agent. The effects after two months of use diminish, according to some of the Russian studies.
Forskolin is a plant native to India that has been used for centuries in traditional Ayurvedic medicine primarily to treat skin disorders and respiratory problems. A considerable amount of research has evaluated the physiological and potential medical applications of Forskolin over the past 25 years. Forskolin has been reported to increase cyclic AMP and thereby stimulate fat metabolism and is used in some sports nutrition formulas.

St. John’s Wart, Kava, Ginkgo Biloba, Ginseng, and L-Tyrosine are believed to serve as naturally occurring antidepressants, relaxants, and mental stimulants and are often included in sports nutrition formulas.
Garcinia cambogia dried fruit rind contains between 10% to 50% Hydroxycitric Acid (HCA), a nutrient that increases fat oxidation by inhibiting citrate lyase and new fat cell formation (lipogenesis).
There is sufficient clinical trial data to support its inclusion in sports nutrition formulas, the calcium salt being the most metabolically active form of HCA.
New products are continually being introduced and marketed in the sports nutrition arena, which is rapidly growing because of health awareness and other factors. The consumer needs to be aware if the new or existing sports nutrition products are based on human clinical data to support their energy or performance enhancement claims.

Maintaining normal, healthy blood sugar levels is a vital part of our physiology, as important as blood lipid management and weight management. Blood sugar is closely linked to the global obesity epidemic we are experiencing, because obese people are at a higher risk of developing diabetes with all its ensuing complications.
In fact, the single best predictor of type 2 diabetes is being overweight or obese. Almost 90 percent of people having type 2 diabetes are obese or overweight. Those who are obese or overweight have greater pressure placed on their body’s pancreatic beta cells to make enough insulin to control blood sugar levels, and this causes the higher risk of developing diabetes.
The reported diabetes cases in the U.S. increased 30% during the 1990’s and greater increases in reported diabetes cases are expected because of the growing rate of obesity.
The next most important factor in blood sugar management is diet, including what we drink. Soda pop manufacturers and the canned foods industry have switched to high fructose corn syrup in the late 1970’s and the beginnings of the obesity rise can be traced back to that time. The reason that fructose or high fructose corn syrup increases obesity is that fructose stimulates lipogenesis in the liver, the formation of new fat cells to a much greater extent than cane sugar (sucrose) does.
Fructose also has a ten times greater potential than glucose itself for causing early glycation products which can then be transformed into Advanced Glycation Endproducts, or AGE’s.
AGE’s are the cross-linking of body proteins, including DNA by aldehydes, compounds that act like a pair of handcuffs that cross-bind proteins in an unnatural, unscheduled way. Scheduled cross-linkage is a natural process of metabolism that is controlled by enzymes.
Scheduled glycation occurs when fructose or glucose molecules are split open by metabolic enzymes so they can be used as fuel for metabolism, but this also exposes two aldehydes in the glucose or fructose molecule that can then cross-link with nearby body proteins.
Unscheduled glycation takes place over a much greater time-period and is the direct, slow direct reaction of glucose with body proteins.
Glycation causes a stiffening of collagen and muscle fibers which we experience during normal aging. This process is accelerated in diabetes. The most serious cross-links occur in endothelial cells, which line the circulatory system and help contribute to atherosclerosis. Cross-linkage of endothelial receptor cells where LDL-cholesterol docks to transport cholesterol, causes a loss of these receptors and an age-related rise in circulating LDL-cholesterol.
Diabetics and persons with elevated blood sugar also have an elevated HbA1c, the measure of how much hemoglobin is glycated.
Blood sugar management strategies include maintaining a normal body weight, which is also measured as body mass index, the ratio of height to weight.
Another important strategy is to limit or eliminate soda pop, sweets, candies and other calorie-dense sugars from the diet.
Several versions of high protein diets have appeared in recent decades and all are based on limiting complex carbohydrate and sugar intake.
Insulin resistance appears to be central to obesity and developing hyperglycemia.
There is a large 79% variance in insulin sensitivity in the general population. There is a well-established relationship between insulin resistance, central fat and abdominal adiposity. These factors are a strong marker and may be a major determinant of insulin resistance in both men and women.
Insulin resistance is also attributed to peripheral insulin resistance, which is the percentage of fat to muscle ratio in the arms and legs. This would seem to indicate that weight training which would increase muscle to fat ratio in favor of muscle, would be a good strategy to decrease insulin resistance.
Drugs like metformin of the biguanide class, are the most widely prescribed oral antidiabetic drugs in the world and are the main line treatment for type 2 diabetes.
However, there are numerous natural compounds that have been used successfully to treat diabetes and hyperglycemia.
Berberine, from the protoberberine family of alkaloids, is mainly obtained from the Berberis aristata plant species, and is widely used in China to treat hyperglycemia. Berberine has been used successfully in 22 clinical trials, only a few of which have been translated and published in Western journals.
Chromium salts, include chromium picolinate and chromium polynicotinate have a large body of clinical trials in hyperglycemia and diabetic studies. More recently, studies using chromium polynicotinate, have had better results in lowering insulin resistance and blood sugar than chromium picolinate, which in two studies, actually increased insulin resistance compared to a control or pretreatment group.
Cinnamon extracts or cinnamon powder from Cinnamomum cassia have considerable clinical data showing a lowering of insulin resistance and blood sugar except in postmenopausal women. The mechanism of action of cinnamon and what active principle or principles are responsible for insulin resistance have not yet been identified.
Ayurvedic traditional medicine has identified several plants and their extracts that have been used to treat diabetes and hyperglycemia.
Pterocarpus marsupium heartwood carved out, filled with water and left standing for some time has been used to treat diabetes described in Ayurveda by the symptoms of thirst and weakness. Modern research has identified (-)-catechin and pterostilbene as active constituents of the plant. (-)-catechin has the unique ability to stimulate the growth of new beta cells on the isle of Langerhans.
Pterostilbene, a close relative of resveratrol, has clinical data supporting healthier body composition in athletes, selective lowering of COX-2 inflammatory enzyme and lowering blood glucose levels.
Other Ayurvedic plant extracts that have hypoglycemic activity include Terminalia chebula, Tribulus terrestris, Shirishadi and Curcuma longa.

Curcuminoids are plant nutrients (also called phytonutrients) that are found in turmeric root (Curcuma longa) — the chief ingredient in curry powder that gives the mixture its yellowish-orange color. Curcuminoids are antioxidants; this means that they neutralize free radicals. The most prominent of the curcuminoids is curcumin.
Free radicals are reactive molecules that are produced by cell deterioration and accelerate the aging processes within the body. Think of them as tiny, invisible sharks zipping around in our cellular seas, taking small electrical bites out of muscle tissue, nerves, and glands. Curcuminoids act as nutritional “police” by deactivating these free radicals so they don’t wreak further havoc in our systems.

The Curcuminoids originate in a herbaceous plant, Curcuma longa that is a member of the ginger family (Zingiberaceae). The best source of this spice comes from Kerala, India. The underground root of turmeric is widely used in culinary dishes throughout the world. Only until very recently, have some of its main components been shown to have medicinal applications as well.
The real strength in turmeric lays in the curcuminoids. There are basically three that we know of right now: curcumin, demethoxycurcumin and bisdemethoxycurcumin.
Besides their already mentioned antioxidants properties, these compounds also manifest anti-inflammatory, anti-mutagen, and anti-cancer activities as well. Inflammation is often due to physical trauma or disease. Numerous experiments conducted on animal models and human volunteers have repeatedly demonstrated wonderful anti-inflammatory action of these curcuminoids. The development of cancer, on the other hand, is a more complex, multifaceted process. Any number of environmental agents, dietary factors, and irregular social behavior initiate chemical stresses of different sorts within the human body. This commences on a cellular level, where such stresses trigger the production of abnormal cells. Curcuminoids have shown the ability to correct this production mistake and soon healthy cells are being formed again.
Curcuminoids have also manifested definite action within the liver several different ways. For one thing, they protect this vital organ from swelling, hardening, and infection. For another, they keep blood which constantly passes through it, flowing evenly which allows better detoxification of the entire organism. Bear in mind that the liver is our major detoxifying organ in the body.
The antibacterial, antiviral, and antiparasitic effects of turmeric root’s principal constituents have also been looked at as well. Interestingly enough, the main curcuminoid, curcumin, has its activities in these areas significantly enhanced with exposure to sunlight. Aflatoxins from ingested moldy food have been significantly neutralized by some of these curcuminoids before they could harm the liver. And intestinal parasites don’t like to stay around very long, on account of curcuminoids presence.
So, what may we deduce from all this information? Simply that curcuminoids help keep us young, cancer-free, and protect against inflammatory disorders like arthritis. Our vital organs, such as the heart and liver are reinvigorated with the strengthening properties of the curcuminoids.
Recent studies by Sabinsa Corporation at leading university in the US revealed that the unique composition of curcuminoids present in Sabinsa’s Curcumin C3 Complex product demonstrated the ability to not only scavenge and neutralize harmful existing free radicals, it was also able to prevent their formation in the first place. An ingredient with such capabilities should perhaps be thought of as more than just another antioxidant. Features such as these merit the term bioprotectant.
To keep your internal self in great shape, the inclusion of Curcumin C3 Complex into product formulations is recommended. Think of curcuminoids as giving your body a whole “new lease on life.” They are readily available, safe to use, and stronger in their effects than many of the other standard antioxidants. No human biological system should be without them.
Curcumin C3 Complex is a registered trademark of Sabinsa Corporation
Patent pending
This product overview was written for the sole purpose of giving a brief history along with educational insights into the product listed above. It is not designed, in whole or in part, as advice for self-diagnosis or self-treatment and should not be construed as such.

For many years the routine medical approach in treating peptic ulcers has been to reduce gastric acidity with antacids or strong drugs which block stomach acid secretion. Two of the world’s best-selling medications for this are Zantac and Tagamet. They are now available in OTC (over-the-counter) versions at somewhat weaker strengths. In prescription form, however, they are much stronger but also more expensive: Zantac at $48.00 for 30 tablets, and Tagamet at $29.00 for 30 tablets. A relatively new third anti-ulcer medication that made its debut in late 1995 is called Prilosec. It is extremely potent and terribly expensive at $104.00 for 30 tablets or a month’s supply.
While they do work for the purpose they’re chiefly intended, namely to halt stomach acid production and thereby give relief to ulcers, all three have some nasty side effects if taken for very long. The number involved reads like a bad laundry list of health dilemmas: nausea, vomiting, constipation, diarrhea, some vitamin and mineral deficiencies, liver damage, hair loss, male breast enlargement, dizziness, allergies, headaches, osteoporosis, depression, insomnia, and impotence.
This is why it is much better to use something natural — an agent that is simple but safe and effective, and inexpensive. The compound referred to is DGL or Deglycyrrhizinated Licorice. The glycyrrhizinic acid component of the root has been removed since it can aggravate hypertension, irritate the kidneys, and induce gout if accumulated in the body for very long. DGL is the preferred form of licorice throughout Europe, much of Asia, and India. But, oddly enough, it is hardly used by herb companies in North America.
A 1982 clinical study tested Tagamet (1 gram daily) and DGL (in the form of Caved-S at six tablets daily) for up to 12 weeks on 100 patients suffering from gastric ulcers. Doctors confirmed that the DGL preparation was “as effective as cimetidine [Tagamet] in gastric ulcer therapy.”
But what would happen if DGL were tested against Zantac and Tagamet? In several head-to-head comparison studies, it was amply demonstrated that DGL was more effective than either Zantac or Tagamet in both short term treatment and maintenance therapy of peptic ulcers. Furthermore, DGL yielded none of the untoward side-effects that the other two drugs did, and did the job of ulcer healing at just a fraction of the cost.
Ulcer sufferers can obtain outstanding help at a fabulous price: two 380 mg chewable tablets of DGL 20 minutes before a meal at less than $25.00 per month! Now that’s a savings worth considering, not only for your pocket book but also for your body as well.
Disclaimer:
This product overview was written for the sole purpose of giving a brief history along with educational insights into the product listed above. It is not designed, in whole or in part, as advice for self-diagnosis or self-treatment and should not be construed as such.

Coleus forskohlii extract (standardized to contain 95% forskolin) is potentially useful in skin care formu-lations, particularly as a conditioning agent. Coleus forskohlii belongs to the Natural Order Labiatae (Lamiaceae), a family of mints and that grows wild in the warm sub-tropical temperate areas in India, Burma and Thailand. In India, it is cultivated for use as a condiment1. In traditional Indian systems of medicine, the roots of Coleus forskohlii are used as a tonic. Other therapeutically relevant properties include anthelmintic action and efficacy in the management of skin infections and eruptions. The plant is also used traditionally in veterinary practice2.
Coleus forskohlii is the only known natural source of the unique adenylate cyclase activating phytonutrient, forskolin3. Adenylate cyclase is the enzyme involved in the production of Cyclic Adenosine Monophosphate (cAMP), a significant biochemical agent in metabolic processes. Cyclic AMP is a “second messenger” hormone signaling system. In many hormone sensitive systems the hormone itself does not enter the target cell but binds to a receptor and indirectly affects the production of another molecule within the cell which then diffuses intracellularly to the target enzymes or a receptor inside the cell to produce the response. This intracellular mediator is called the second messenger. cAMP and therefore forskolin have marked physiological effects through such “second messenger” actions on various biochemical processes in the body. A recently patented application includes the potentiation of lean body mass and benefits in the management of mood disorders4. Potential topical applications include its role as a skin-conditioning agent to support localized fat loss on topical application5.
Research carried out over the last few decades has revealed the multi-faceted pharmacological effects of forskolin. Most of these effects have been linked to the role of forskolin as an activator of adenylate cyclase7.
The spectrum of potential therapeutic activities is represented in
Adenylate cyclase is also involved in the regulation of lipolysis or enzymatic breakdown of fat in the adipocytes (fat cells). Hormone sensitive lipase mediates lipolysis and this enzyme is activated through phosphorylation by protein kinase A that in turn is activated by cAMP.
Topical fat reduction in specific areas of the body is a common concern for women. Ronsard8 popularized the term “cellulite” to describe the dimpling and “orange peel” external appearance of the thighs, the cause of which was attributed to the aging process by later researchers9. The structure of subcutaneous adipose tissue accounts for the development of the “orange peel” appearance. Groups of fat cells are attached to the underside of the dermis by fibrous connective tissue. As fat cells enlarge, the fibers are stretched and pull down on the underlying skin. This causes the indentation or dimpling of the skin called cellulite.
The adrenoreceptors play important roles in the regulation of lipolysis. Adrenoreceptors are neurons that are activated by adrenaline (epinephrine) or similar substances. The relative number of b-2 and a-2 adrenoreceptors on the surface of the fat cells determine the balance of lipolysis in those cells. Hormones such as estrogen influence the number of a-2 and b-2 adrenergic receptors in the fat cells. Through the effects of estrogen, women more a-2 adrenergic receptors in fat cells in the hip and thigh region12. The a-2 adrenoreceptors and the adenosine receptors in fat cells stimulate specific proteins [GTP inhibitory binding proteins (Gi proteins)] that inhibit adenylate cyclase thereby inhibiting lipolysis. A healthy balance of lipolysis is maintained through the simultaneous action of the b-2receptors that activate specific proteins [GTP binding proteins (Gs proteins)] which in turn activate adenylate cyclase (and thereby cAMP), stimulating lipolysis. Due to the increased number of a-2 adrenergic receptors in the hip and thigh region in women, fat mobilizaton becomes more difficult from these areas5. b-adrenergic stimulation and a-2-adrenergic inhibition has been reported to increase lipolysis from fat cells13.
It has been demonstrated that adipose tissue metabolism varies from one region of the body to another, for example, in severely obese women losing weight after the jejuno-ileal bypass surgery, fat was seen to be absorbed more slowly in the thigh region than the abdominal region10. These differences lead to the hypothesis that localized application of agents that trigger lipolysis or fatbreakdown could help in cases of fat accumulation at specific subcutaneous sites4. Forskolin accelerates lipolysis through the activation of hormone-sensitive lipase11
Forskolin bypasses the adrenoreceptors, increasing cAMP levels directly, thereby stimulating lipolysis. The beneficial effects of forskolin, therefore, do not depend upon the sensitivity of the adrenergic receptors, which can often decreases with age and other physiological factors. Forskolin has also been shown to counteract the decreased response of fat cells to epinephrine, associated with aging.
A clinical study performed in 198713 established that regional fat loss from the thigh in obese women could be effected through adrenergic modulation. In this study, twenty eight obese women were placed on a calorie-restricted diet and subjected to one of five topical treatments to one thigh three to five times per week for four weeks: (1) isoproterenol injections; (2) cream containing forskolin, aminophylline, and yohimbine; (3) yohimbine cream; (4) forskolin cream; or (5) aminophylline cream. The opposite thigh was treated with a placebo (injection or cream), serving as the control. The treated thighs lost significantly more girth after treatment (both by injection and by cream). Additionally, no adverse reactions were observed that could be attributed to either the cream or the injections. The authors of this study concluded that local fat reduction from the thigh could be safely accomplished, using agents that affect the adrenergic mechanisms.
In a double–blind clinical trial5, five overweight women were treated with an ointment containing forskolin (1.2 X 10-5 mol/L), yohimbine (2.5 X 10-4 mol/L) and aminophylline (1.3 X 10-2 mol/L) in an aquaphor base on one thigh or the base alone (placebo) on the other thigh, for four weeks, five days per week. The subjects’ thighs were wrapped with warm 600 to 900 mOsm/L magnesium sulfate solutions for 30 minutes prior to each application to maximize transcutaneous absorption. An occlusive plastic wrap was placed over the area to which the ointment was applied for the entire study period.
Measurements of girth two-thirds of the way between the knee and the greater trochanter were used to measure fat loss at the end of the study period. Treated thighs showed significant decrease in girth fat loss as compared to untreated thighs with no significant changes in total body weight
The decrease was attributed to the combined actions of forskolin, aminophylline and yohimbine that effected localized fat loss by different mechanisms – forskolin through cAMP and b-2 adrenoreceptor activation; aminophiline through adenosine receptor antagonistic action and inhibition of phosphodiesterase and yohimbine through a-2 adrenoreceptor antagonistic action.
A subsequent trial5 studied the effects of the individual components of the ointment. Eighteen women were divided into three groups of six each, each group receiving one of the active compounds. The women were placed on a 800 kcal/day diet and encouraged to engage in a walking program. As before, the warm wraps with magnesium sulfate were applied, but the occlusive plastic wrap was not used. Six women had one thigh treated with an ointment containing 25 X 10-5 mol/L forskolin in aquaphor base while the other thigh was treated with the base alone. Thigh girth measurements were taken as before. Four of the six women completed the study and showed significant decrease in treated thigh girth (p < 0.05) as compared to the untreated thigh (Figure 4).
The authors of this study concluded that localized fat loss could be effected through topical application of substances like forskolin that stimulate lipolysis.
The subcutaneous fat cells are stimulated first, the dimpling on the skin of the thigh is lost as tension is relieved on the connective tissue that attached to the under surface of the dermis.
Based on these clinical studies reported in literature, Coleus forskohlii extract 95% is potentially useful in dislodging localized fat deposits immediately under the skin, when applied topically. The recommended levels of use as a skin conditioning agent : 0.1 to 0.5% of a topical formulation, such as an ointment, cream or lotion. To improve transdermal penetration of the extract, 0.01-0.1% CosmoperineÒ (a standardized preparation derived from black pepper, a registered trademark of Sabinsa Corporation)14 may be added to the formulation.
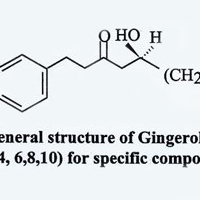
Ginger is a well known spice and flavoring agent which has also been used in traditional medicine in many countries. This large seasonal plant is cultivated in Southeast Asia and China, India, and some parts of Africa. Ginger and turmeric plants have several similar characteristics – both possess pale green flowers and are surrounded by long lanceolate leaves.
Ginger, a source of valuable phytonutrients, is characterized as having an aromatic odor and a pungent taste1. The part of the ginger plant that is used is the root, which is botanically the rhizome. The flat surfaces of the rhizome are removed, leaving the remains of the underground stem2. Ginger contains essential oils including gingerol and zingiberene. It also contains pungent principles such as zingerone, gingerol and shogaol3.
For centuries, in Ayurvedic and Tibetan systems of medicine, ginger has been used in the management of headache, nervous diseases, nausea, and vomiting. Ginger has been noted to treat migraine headaches without side-effects4. In addition, it is also recommended in the management of rheumatic disorders and muscular pain5.
The ginger rhizome has the following chemical composition:
The percentage of essential oil varies with geographic origin. However, its chief elements, sesquiterpene hydrocarbons, remain constant. These include (-)-zingiberene, (+)-ar-curcumene, (-)-ß-sesquiphellandrene, E, E- a -farnesene, and b -bisabolene. These essential oils occur alongside monoterpene alcohols and aldehydes present as glycosides. A mixture of many terpenes and some non-terpenoid compounds make up the essential oil.1 It has been speculated that since there are a variety of chemical classes that these compounds can belong to, it is likely that ginger can eliminate symptoms associated with a variety of illnesses, such as arthritis, by interfering with the production and release of metabolic products from lipid membranes, peptides, proteins and amino acids.
Experimental data reveal that ginger may be a dual inhibitor of eicosanoid synthesis, inhibiting the synthesis of both prostaglandins and leukotrienes, which are inflammatory mediators produced from arachidonic acid5.
The rhizome contains a variety of chemicals called gingerols which provide its distinctive taste and characteristic pharmacological effects. The chemical constituents responsible for the pungent taste of ginger are 1-(3’ –methoxy –4’-hydroxypheny1)-5-hydroxyalkan- 3-ones, also known as [3-6]-,[8]-,[10]-,and [12]-gingerols.1
In recent years, researchers have scientifically validated many of the therapeutic uses of ginger.
Many anitihistamines are used to treat migraines. Ginger has been shown to contain antihistamine and antioxidant factors as well as possess anti-inflammatory action4.
The above studies indicate the inhibitory effects of ginger on synthesis of inflammatory mediators and the beneficial effects of powdered ginger as well as the isolated gingerols on digestion and metabolism. In view of these effects, ginger is a potential herbal alternative in the management of digestive disorders, migraine, painful arthritic conditions and motion sickness. The herb may be potentially useful in improving blood circulation as well, on account of its inhibitory effects on platelet aggregation. When used as a spice or therapeutically at the recommended levels, [for motion sickness: 300 mg of the extract (containing 5% gingerols) daily in divided doses; for digestive distress: (75 mg of the extract daily in divided doses)], ginger does not have any reported side effects7.

Glucosamine (chemically 2-amino-2-deoxyglucose), commonly known as chitosamine is currrently recognized as a safe and effective antiarthritic agent1. It is found in mucopolysaccharides and mucoproteins, which form the frame work of vertebrate connective tissues. It occurs extensively as chitin in the exoskeleton of invertebrates, including arthropods and marine organisms. Microbes such as yeast and other fungi also contain chitin. Chitin is a biopolymer made up of units of N-acetyl-glucosamine. Glucosamine can be isolated from chitin or prepared synthetically. For pharmaceutical use as an antiarthritic agent, glucosamine is supplied in the form of products such as glucosamine sulfate.
Glucosamine sulfate is the preferred form of glucosamine for therapeutic use, mainly as an antiarthritic agent. It is an effective means of providing glucosamine orally, as a building block for the regeneration of cartilage glycosaminoglycans, lost during the progression of osteoarthritis.
Each unit of glucosamine sulfate contains two molecules of glucosamine as below:
In vivo, glucosamine sulfate breaks down into glucosamine and sulfate ions.
Cartilage glycosaminoglycans are formed from glucosamine. Glucosamine is biochemically generated in the body from fructose-6-phosphate, a product of glycolysis. The glucosamine formed is converted to galactosamine, which is then incorporated into glycosaminoglycans and glycoproteins, the building blocks of cartilage tissue.
During the progression of osteoarthritis, there is substantial degeneration of cartilage glycosaminoglycans. The availability of glucosamine, a critical intermediate in the synthesis of mucopolysaccharides in cartilage tissue, is rate limiting for proteoglycan production. Glucosamine administration could therefore be expected to induce the formation of glycosaminoglycans, thereby restoring the depleted glycosaminoglycans and proteoglycans. The anti-inflammatory activity of glucosamine sulfate have also been reported by several researchers. The following effects of glucosamine sulfate have been proven in several detailed studies:
Preclinical studies were directed at understanding the mechanism of action of glucosamine sulfate as an antiarthritic agent and its safety during subacute or chronic administration.
The antiarthritic effects of glucosamine sulfate are best described as being linked to its antireactive properties. The mechanism of action is therefore thought to be different from that of conventional non steroidal antiinflamatory drugs. Unlike conventional NSAIDs, Glucosamine sulfate acts by stimulating the synthesis of proteoglycans which stabilize the cell membranes and the intercellular substance. In view of this mechanism of action, glucosamine sulfate can be said to have antireactive rather than antiinflammatory properties. Glucosamine sulfate has cyclooxygenase-independent antireactive properties and no analgesic action.
The comparative protective effects of glucosamine sulfate and indomethacin are shown in Table 1:
Table 1 : Inhibitory concentrations on mediators of inflammation (concentrations able to inhibit the investigated mediator by 25% (IC25) or by 50% (IC50) 1
Model |
Glucosamine sulfateIC (mmol/l) |
IndomethacinIC (mmol/l) |
| Rat : proteolytic enzymes in inflamed paw | IC25 > 3 | IC25 0.33 |
| Rat : lysosomal enzymes of
the liver |
IC25 3 | IC25 0.27 |
| Superoxide generation | IC25 > 3 | IC25 0.07 |
| Inhibition of prostaglandin synthesis
¾ Stimulated by arachidonic acid |
IC50 > 660 | IC50 0.50 |
| ¾ Stimulated by histamine | IC50 > 660 | IC50 0.53 |
From the above table, it may seem that glucosamine sulfate shows a very low potency as compared to indometacin. However, glucosamine sulfate has very low toxicity making it more suitable for long term administration. The LD50 values for oral administration of glucosamine sulfate, indometacin and acetyl salicylic acid are shown in Table 2:
Table 2 : LD50 values by oral route
| Substance | LD50 values (mg/kg) by oral route | |
| Rat | Mouse | |
| Glucosamine | > 8000 | > 8000 |
| Indometacin | 12.3 | 12.8 |
| Acetyl salicylic acid | 1435 | 1050 |
The antireactive activity of glucosamine sulfate was tested in rats8 with experimental models such as:
a) sponge granuloma and croton oil induced granuloma (subacute inflammation)
b) kaolin arthritis (subacute mechanical arthritis)
c) Immunological reactive arthritis
d) Generalized inflammation (adjuvant arthritis)
Glucosamine sulfate was found to be effective in oral daily doses of 50 to 800 mg/kg. The potency of glucosamine sulfate in comparison with that of indometacin in the same tests was found to be 50-300 times lower. However, toxicity of indometacin in chronic toxicity experiments was found to be 1000 to 4000 times larger. The therapeutic margin with regard to prolonged treaments required for inflammatory disorders results 10-30 times more favorable for glucosamine sulfate than for indometacin. Based on these observations in animal models, glucosamine sulfate is evidently the drug of choice for prolonged treatment of inflammatory disorders8.
Additionally, the anti-viral properties and anti-cancer properties of glucosamine have been investigated and its inhibitory effects on a carcinoma have been demonstrated5. Currently, however, the focus is on the use of glucosamine sulfate in the management of rheumatic disorders.
| EFFICACY OF GLUCOSAMINE SULFATE (INTRAMUSCULAR, 400 mg, twice a week for six weeks) IN THE TREATMENT OF OSTEOARTHRITIS OF THE KNEE AS COMPARED TO PLACEBO |
Rationale behind the preferential use of Glucosamine sulfate over Glucosamine hydrochloride:

Tea is an infusion of flavorful leaves that has been consumed for centuries as a beverage and is valued for its medicinal properties. Today, scientific research has validated its healthful effects and the cup that cheers has gained recognition as the cup that heals.
The tea shrub (genus Camellia, family Theaceae) is a perennial evergreen with its natural habitat in the tropical and sub tropical forests of the world. Cultivated varieties are grown widely in its home countries of South and South East Asia, as well as in parts of Africa and the Middle East. The young shoots or flushes are plucked and processed into green (unfermented), black (fermented), oolong (red, partially fermented) or yellow (partially fermented) teas. In fermented teas, the action of leaf oxidizing enzymes, (mainly aka polyphenol oxidase) convert the tannins and catechins in tea leaves into brown/red colored products1.
Green tea (Camellia sinensis) has been acclaimed for its antioxidant properties, attributed to the presence of catechins such as epigallocatechin gallate (EGCG). These compounds promote health by preventing lipid oxidation and have been proven to possess antibacterial and antiviral action as well as anticarcinogenic and antimutagenic properties.
The catechins in green tea are responsible for its medicinal properties2.
Other biologically active compounds present in green tea include the methylxanthines, theophylline, theobromine and caffeine. Theophylline has been used as a bronchial smooth muscle relaxant in the treatment of asthma and bronchitis.
The biological benefits associated with green tea catechins especially epigallocatechin gallate, are generally attributed to their antioxidant activity2. They are also reported to scavenge free radical oxygen3. In studies with lard or vegetable oil, the tea catechins were found to reduce the formation of peroxides more effectively than dl-a-tocopherol or BHA. The antioxidative activity increased in the following order: EC<ECG<EGC<EGCG. In view of these results, the potential use of the catechins in green tea as effective natural antioxidants in foods has also been explored.
Tea catechins are believed to act as anticancer agents by detoxifying cancer causing substances in vivo 4,5. In vitro studies revealed that catechin gallates selectively inhibit 5 a-reductase. This enzyme is responsible for the conversion of testosterone to 5-a dihydrotestosterone6. 5-a dihydrotestosterone at high levels, has been implicated in the etiology of prostate cancer and male pattern baldness.
The anticarcinogenic effect of green tea extract was studied on mouse skin. Green tea catechins, especially EGCG inhibited each step in the conversion of a cancer to malignancy. Tea was also found to offer protection against chemically induced tumor initiation, promotion and progression to malignancy as well as inhibit skin cancer induced by ultraviolet radiation7.
In mouse models of chemically induced lung and stomach cancer, there was significant inhibition of tumor incidence and proliferation when green tea catechins were orally administered. Oral administration of 0.012-1.25% of EGCG or green tea extract to mice or rats with chemically induced oesophegal, intestinal, colon, liver and mammary tumors was found to have a potent inhibitory effect on carcinogenesis.
Recent studies showed that tea drinking reduced the risk of oesophageal cancer in Chinese women; oral cancer in northern Italians; gastric cancer in Swedish adolescents; pancreatic cancer in elderly Poles and residents of a retirement community in the U.S.; and colon cancer amongst retired male self-defense officials in Japan. It is now generally accepted that tea drinking has chemopreventive effects8.
Green tea catechins have been shown to be antimutagenic, lowering the formation of heterocyclic amines9 (formed during the cooking of meat and fish and proven to be mutagenic). They have also been shown to reduce the occurrence of chromosome aberrations during mutagen exposure10.
Lipid peroxidation especially the oxidation of LDL (Low Density Lipoprotein) has been implicated in the etiology of atherosclerosis. In vitro studies confirmed the inhibition of lipid peroxidation induced by cupric ions, by green tea catechins. Green tea extract was found to prevent the increase in serum cholesterol in mice fed high fat diets. A recent cross-sectional study also revealed that in people consuming more than ten cups of green tea per day, there was decrease in serum cholesterol levels, decrease in LDL, VLDL (Very Low Density Lipoprotein) and triglycerides, increase in HDL and reduction in atherogenic index. In the same study, tea consumption was also found to decrease the levels of serum markers of liver damage11. In a study on an elderly group in the Netherlands suffering from coronary heart disease, tea (probably not green tea) was found to reduce the risk of death from this condition12.
The catechins in green tea were also found to inhibit hypertension in mice (resulting from chronic psychosocial causes) through enhanced sedative action of the brain neurotransmitter GABA 13, gamma amino benzoic acid. Green tea was also found to lower the incidence of stroke in the elderly14.
The tea catechins (particularly EGCG and EC) were found to have bactericidal properties. They are believed to damage bacterial membranes. Tea has been used in the treatment of diarrheal diseases and infections such as cholera and typhus15. Green tea is also believed to have protozoacidal and virucidal16 (including HIV18) properties. However, the effectiveness of tea catechins in the treatment of human viral diseases needs to be confirmed. EGCG has also been shown to stimulate the immune response, in studies on mice. In this case, the galloyl group in EGCG was postulated to stimulate mouse splenic B-cell proliferation19.
Green tea catechins are believed to offer protection against tooth decay by three mechanisms:
Tea drinking may promote longevity, as evidenced by the low mortality rates amongst Japanese females who are traditional practioners of the tea ceremony22.
Green tea by virtue of its scientifically validated healthful effects has potential utility in the management of a variety of disorders. This ancient herb, associated with wakefulness and harmony in Buddhist legend, has now found its rightful place in modern alternative medicine as a versatile healer.

If you are looking to burn more body fat, gugulipids could be the plant extract for you.
Stroke is the third leading cause of death in North America and Europe, just behind coronary heart disease and cancer. When it happens, it can either be a little one (actually a series of undetected petite strokes over a given period of time) or else, more often than not, one of major consequence that can leave in its wake temporary paralysis and partial amnesia, among other things.
A stroke is initiated with the formation of a blood clot. A clot forms when blood platelets become too sticky and start clustering together like a bunch of grapes. When this happens, the flow of blood starts slowing down in a process similar to 5:00 p.m. traffic backup on the freeway systems of many of America’s major cities.
Gugulipid also has demonstrated in more than two dozen clinical trials, its incredible lipid-lowering properties. It not only lowers total serum cholesterol and plasma triglycerides, but also greatly reduces “bad” cholesterol (LDL-cholesterol), while at the same time increasing “good” cholesterol (HDL-cholesterol). This should come as welcomed news to those who worry about their heart arteries or livers becoming clogged up with too many fat deposits.
Another remarkable accomplishment of Gugulipid is its ability to accelerate the chemical “burning” away of stored fat, by simply converting it into more physical energy. This is done by resetting the body’s own “fat thermostat” a few degrees higher (not to be confused with an unhealthy rise in body temperature). All of this action takes place in the thyroid, that butterfly-shaped gland that sits atop the windpipe at the base of the neck. When Indian scientists administered an isolated ketosteroid from gum guggul to animal models, they noticed, according to their report, “a significant increase in all the thyroid functions” of these rodents. And slightly accelerated thyroid activity with Gugulipid means an increase in the body’s overall metabolic rate, or heightened internal combustion of stored fat.
Gugulipid, in combination with several other plant ingredients of Ayurvedic origin, was studied in humans also. The results of the various formula combinations showed positive effects for weight loss. Gugulipid was the main ingredient in all four combinations studied.
Gugulipid is safer than much of the water we drink or air we breathe these days. It is extremely user-friendly to all body systems and will do our internal vital organs much good if taken in moderate amounts (2 capsules or tablets) each day with a meal of some kind.
$34.99

$25.99
$7.99

$23.39